Last time we spent a great deal of time looking into the characteristics of long bones with an eye towards which ones make good targets. Let's continue the discussion and work through the rest of the list of easily-damaged structures which we previously identified.
Bridge Of The Foot
The bridge of the foot didn't show up in our inventory of breakable bones in Part I because none of the bones of which it is comprised are ideal candidates under the criteria we outlined. The metatarsals are thin, but they're also short and thus difficult to break. Similarly, the bones of the bridge proper (naviculus, talus, etc.) are thick and round, about the exact opposite of ideal. However, because the foot is the base of the pillar which is the leg, it spends a lot of time in direct contact with the ground. This makes the foot a good target for the following reasons:
- Anyone with any degree of flexibility can strike the foot.
- Gravity is on the attacker's side: Done correctly a strike to the bridge of the foot is backed by most of the attacker's mass.
- It's hard to move the foot at will: Generally at least one foot must remain planted at all times.
- The ground is the worlds best brace; it completely prevents the foot from recoiling from a strike.
- It's really hard to fight with a broken foot.
That said, it's also important to note that getting in close enough to effectively strike the foot is dangerous business. As such it's a target of opportunity; go for the foot if you find yourself in close, but don't close in just to attack the foot.
There are two main types of injury which are typically inflicted by a strike to the foot, either a fracture of the metatarsals or a Lisfranc Fracture/Dislocation, depending on where the strike actually lands. The former is painful but rarely disabling while the latter, if serious enough, will prevent the foot from bearing weight1, recommending that, if you find yourself in the position to choose, you aim for the bridge proper rather than the toes.
Interestingly, strikes to the foot are greatly affected by the type of footwear which one is wearing. In the classic case, fighting bare-footed, a strike to the foot is usually delivered via the attacker's heel3 which, since the heel is a blunt, rounded instrument, spreads the force out over a fairly wide area. Compare this with the scenario where you take after someone with the heel of your cowboy boots. The heel of a boot has a sharp edge and thus distributes the force over a relatively narrow area; it's going to do a lot more damage.
So what about the vital points associated with the bridge of the foot, the koori and uchi kuro bushi? Searching for "koori acupuncture pressure point" turns up two sources, here and here, though the latter appears to be a copy of the former. Reading the material presented on the koori should give you a good sense of why I took up writing this blog:
13. RESULT: Fainting , Senseless, severe pain to the foot and the loin, by stimulation to the inner foot nerve and shin artery and bone nerves, causing loss of motor organ.
Uh-huh... and than only happens if I strike a point 0.3 - 0.5 (in? cm?) deep between the first and second toes? A good strike to anywhere on the bridge of the foot will result in pain to the foot, could cause shooting pains up the inside of the leg, and may result in the foot becoming non-functional. And there's bugger-all in terms of body systems in that area, no nerve bundles or lymph nodes or anything else that could possibly cause unexplained, knock-on effects. Why invoke an "energy meridian" when the result being described is easily explained using basic physiology? And it gets better...
14. CURE: In the case of a light press (tread), massage then use ice pack. If hit heavily (crush) medical help will be needed.
Translation: "If someone steps on you foot, get an icepack. If someone really steps on your foot, get a doctor". Uh... duh? If the injury is caused by a disruption of the flow of chi doesn't that imply that the appropriate remedy is to undue the disruption, maybe by humming or something? Anyway, it's the same deal with the uchi kuro bushi... the only relevant results for a search on the term are this blog and pressurepointkarate.com. I love the description they provide:
15. RESULT: Certain, long term slow death.
16. CURE: None, what so ever.
Let's stop and think about this claim for a second. People get sick and die all the time whether or not they've been jabbed in the foot. It would take a tremendously large number of observations to establish a correlation between being struck in the uchi kuro bushi and "certain, long term slow death". I'll go so far as to say that there's absolutely no way that anyone has actually observed such a correlation; any support that can be mustered will be anecdotal and likely subject to selection and/or recall bias. So, as far as the uchi kuro bushi goes, I'm going to call bullshit and chalk it up as one more example of the credulous transmission of dogma.
Tailbone (Coccyx)/Bitei
The tailbone (or coccyx) is a vestigial structure left over from when we used to have tails. It's not load-bearing nor does is serve any secondary function; it's basically just hanging out not doing much of anything. If you fall on your backside hard you might end up breaking it, which will probably hurt and may impair mobility, but that's about it.
In my humble opinion it makes a piss-poor target. You can only reliably strike the coccyx if your opponent is facing away from you, but if you find yourself in that position there are lots of targets to go for that'll get you a better return. Even if you do manage to fracture someone's coccyx it's likely not going to slow them down all that much, so don't bother.
So let's look at the associated striking point, the bitei. A google search on the words "bitei striking point" does turn up a number of relevant hits, the majority of which simply define "bitei" as "coccyx" without further discussion, though it's more specifically defined as the tip of the coccyx here and here. The Pressure Point Karate people give this description:
11. RESULT: Long term pain in any case, due to pressure, fracture or breaking to the tip of the Coccyx. The length of time of pain in any case can last from weeks to years.
12. CURE: The tip of the Coccyx, is one of the bodies shock absorbers, and can be easily broken. May or may not heal on it’s own, unless broken, In the case of a complete break, medical help would be necessary.
Again, I'll point out that they aren't describing any effects that can't be explained by "dude, you broke your butt".
The Ear And Related Bits
I had initially thought to treat the hinge of the jaw (aka "mandibular condyle"3), the ear, and the mastoid process separately but I realized that, from the standpoint of target selection, they're basically all the same thing. If you aim for any one of the above you may very well hit one of the others given that your opponent will generally present a moving target. So it's probably better to treat the entire area around the ear as one large target and then talk about the different ways it can be damaged.
A blunt-force strike to this area can result in any of the following:
- Rupture of the eardrum (tympanic membrane) and/or longitudinal fracture of the temporal bone, both of which can lead to hearing loss and possibly dizziness4.
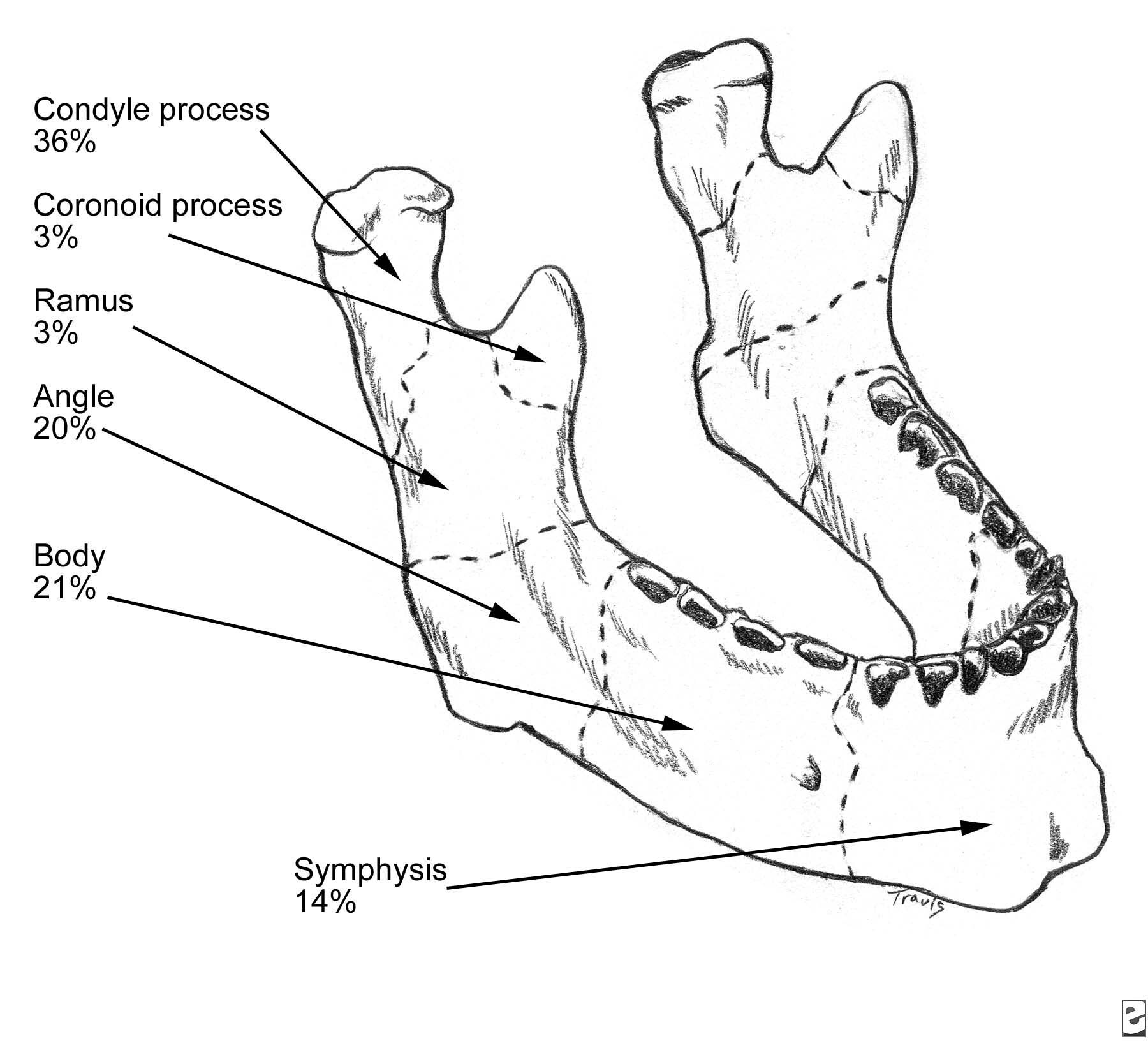
- Fracture of various portions of the jaw (mandible), usually the condyle or mandibular angle5, leading to jaw pain and/or numbness.
- Swelling and hematoma of the ear proper (pinna)6.
{kind=link}
It's also possible to punch someone hard enough to fracture their cranium7, but it would be extremely unusual for that to happen in the context of typical standing combat. Note that I've said nothing about any knock-on (pardon the pun) effects such as concussion; I'll deal with those later in a separate post.
There's not much cause to go after the jaw or the ear itself. A fractured jaw is an annoying distraction, but its not going to put someone out of commission. Likewise, having your ears boxed is unpleasant, but its the type of injury that you might not even notice until after the fact. The real winner here is the eardrum; an open-handed strike which cups the ear can increase the pressure in the outer ear to the point where the eardrum ruptures. Such a strike is close to ideal from a self-defense perspective: it doesn't take a lot of strength or flexibility to execute and can cause significant, but short-term and reversible, disruption to your opponent.
Eye/Seidon
Not much to say about this; the eye is soft and easily damaged. Strikes to the surrounding bone and tissue can lead to a black eye which, if severe enough, will effectively force the eye closed in a very short time. Poking the eye itself can, in the most extreme cases, rupture the eye leading to blindness. As far as the seidon goes it looks like more of the same; it basically amounts to "strike the eye hard enough and you can cause unconsciousness". Well... duh again.
Nose
Last, but not least, is a mass of cartilage and a little bit of bone that you and I know as "the nose". Of all the facial bones the nose is most often broken because it is a) fragile, b) protuberant, and c) situated right in the middle of the face where someone is just bound to come along an punch it8. Between the accompanying bleeding and the swelling a broken nose can be, in the very least, somewhat distracting; a really severe fracture can prevent you from breathing through your nose entirely. There's zero question that the nose is a highly effective area to target though, contrary to popular belief, hitting someone's nose isn't going to drive spikes of bone into their brain.
1 http://www.rushortho.com/ot_foot.cfm
2 The ball of the foot can be used as well but, because the foot pivots at the ankle, that will always be less effective than striking directly with the heel.
3 Which I've previously referred to as the "capsular ligament", though that designation is slightly inaccurate. The actual hinge of the jaw is the condyle; the capsular ligament connects the condyle to the skull.
4 http://www.utmb.edu/otoref/Grnds/Trauma-ear-021023/Trauma-ear-021023.htm
5 http://emedicine.medscape.com/article/84613-overview
6 http://emedicine.medscape.com/article/1283150-overview. This type of injury leads to cauliflower ear in the long run.
7 http://www.astm.org/JOURNALS/FORENSIC/PAGES/JFS2002024_482.htm
8 http://www.merck.com/mmpe/sec21/ch312/ch312d.html